
Abstract
Introduction
Cancer cases are rising globallywith a noticeable rise in younger adults. Screening and early detection are effective in decreasing mortality. Workplaces can play a role in promoting cancer screening uptake. This systematic review investigated the effectiveness of workplace breastlungcolorectaland cervical cancer screening interventionsand the factors impacting their effectiveness.
Methodology
Six databases (EmbaseMedlineWeb of ScienceCINAHLCochrane LibraryScopus) were searchedand cancer screening promotion and cancer screening uptake was analysed using effect direction plots. Magnitude of effectiveness (i.e.change in knowledge or screening rate) was also evaluated.
Results
In total13,426 articles were identified. After screening and applying the eligibility criteria21 articles were included in the analysis. A positive effect direction was seen for all workplace cancer screening promotion interventions. Magnitude of effectiveness for cancer screening promotion interventions resulted in a > 30% change in knowledge or screening uptake in 4/7 of breast cancerin 3/4 of cervical cancer and 1/3 colorectal cancer screening promotion interventions. For workplace cancer screening uptake interventionsa positive effect direction was observed for the majority (18/22). Cancer screening uptake interventions showed a > 30% change in magnitude of screening rate in 4/7 breast cancer5/10 colorectal cancer and in 1/5 cervical cancer workplace interventions. No studies for lung cancer were eligible. Factors positively influencing effectiveness included an interest in health and previous healthcare usewhile fear of cancer and embarrassment of screening negatively influenced effectiveness.
Conclusion
Workplace cancer screening promotion and uptake interventions can effectively improve cancer screening knowledge and increase uptake of screening tests.
Similar content being viewed by others

Introduction
Screening for cancer and precancerous lesions can improve the chance of recovery and slow progression of the disease if detected early [1,2,3]. Cancer screeninghoweveris not without side effectsand thereforeroutine cancer screening tests with the lowest harm and highest benefits are recommended for specific age groups and time intervals [24] (Appendix A). Despite the recommendations and programs in placescreening coverage varies widelyand even high-income countries struggle to increase and maintain screening coverage. In the United States (U.S.)median screening rates in 2020 for mammography and colorectal cancer were 71% (eligible ages: 50 to 74 years) and 59% (eligible ages: 45 to 75 years)respectively [5]. In England68.7% took up breast cancer screening (eligible ages: 50 to 71 years)and 65.9% (eligible ages: 60 to 74 years) were adequately screened for colorectal cancer between 2019 and 2020 [6].
Even though the prevalence of most cancers is higher in older populationsit can occur at any age [7]. A noticeable shift in cancer incidence is seen as cancer becomes more common in younger generations [8]. In 2020new cancer cases for all cancers in the working-age population (15–69 years) were 11 millionmore than half of the total diagnoses worldwide [8]. The United States Preventive Services Task Force (USPSTF) reported that from 2000–2 to 2014–16a rise of ~ 15% was recorded in colorectal cancer incidence in people aged 40–49 years [9].
Along with this trendthe burden of cancer on the working population becomes more extensiveimpacting every aspect of their lives [10]. Cancer can heavily impact work ability [11,12,13,14,15]financial stability [10]and productivity [11,12,13,14,15]resulting in difficulty securing and maintaining employment for cancer patients or those recovering [1617]. Furtherthose returning to work may endure additional challengessuch as discriminationbiasor even layoffs if they are considered incapable of performing their jobs effectively [18]. It is evident that the burden of cancer extends beyond the individualto their familiesemployers and society as a whole [16].
Workplacesas a settingcan affect change in public health and in individual behaviours [19]and can be used to strengthen cancer screening engagement [2021]. Workplaces can provide easy and regular access to people from various sociodemographic and economic positions [20] and influence screening behaviour [22] by providing positive social normsa convenient setting for screeningremoving structural barriers for employees and promoting health education [1923]. Workplace incentives can also motivate employees to take up screening services [21]. Employers on their sidehave motives to implement interventions targeting employee wellbeingas they have a responsibility to protect and prioritise the health of their employees by implementing health and safety regulations and by promoting healthy behaviours [24]. For working environments that are considered to be exposing their employees to known cancer risksincluding carcinogenssedentary lifespsychological distressand shift workemployers and organizations may be considered partially responsible for providing cancer screening [25].
To our knowledgeworkplace cancer screening intervention studies to date have only examined single workplacesor single or two cancers at a time. Thereforethis study aims to undertake a systematic review to assess the effectiveness of workplace cancer screening promotion and cancer screening uptake interventionsas well as the factors that can facilitate or hinder engagementuptake and the effectiveness of these interventions.
Methodology
The protocol for this review was registered in PROSPERO (CRD42022334827).
Research Questions:
1. Are workplace cancer screening promotion interventions and cancer screening uptake interventions effective?
2. What are the factors that influence engagementuptake and the effectiveness of these interventions?
Workplace cancer screening promotion and screening uptake interventions
We focus on cancer screening promotion and screening uptake interventions for four common types of cancer with recommended screening tests by the USPSTF: breastlungcolorectumand cervix uteri [926,27,28]. Prostate cancer screeningalthough the prevalence is highwas not included as this is not recommended for population-based screening [29]. During the literature reviewwe considered the screening recommendations by reputable organizations including the World Health Organizationthe United States Preventive Services Task Force (USPSTF)the National Health Service of the United Kingdom and the American Cancer Society. In the endwe chose to use the USPSTF recommendations as the base guideline since it has the broadest and most clear range of recommended ages and screening investigationswith regular updates. Workplace cancer screening promotion interventions were defined as interventions promoting knowledge and information on existing cancer screening serviceswithout offering physical screening tests by workplaces or researchers. This may promote the use of existing national screening programs or individual out-of-pocket screening uptake. Examples of cancer screening promotion interventions are health talks on breast cancer screening at workplaces and allowed paid time off to attend screening. Cancer screening promotion interventions were included in the review as some workplaces may only be able to promote cancer screening because firstlythe availability of cancer screening services varies depending on each country’s health system (e.g. in the UKNational Health Service (NHS) screening services are available to all eligible citizens)[30]and secondlyassociated costs may render screening tests prohibitive for workplaces.
Workplace cancer screening uptake interventions were defined as interventions in which employees were offered cancer screening services by workplaces or by researchers in workplaces as another screening opportunity additional to the national programs or individual screening in the private sector (e.g.providing cervical cancer self-screening test kits to the employees at work). The workplace interventions included could be organised by the employer or by an external agency but supported by the workplace.
Search strategy
The search strategy was generated by combining three core concepts: (i) workplace settings and/or interventions organised by workplaces; (ii) cancer; and (iii) the four sites of common cancers and screening tests. Search terms were developed for each conceptusing truncationsBoolean and proximity operatorsand Medical Subject Headings (MeSH). Pilot searches were conducted to balance a good level of sensitivity and specificity in identifying relevant articles. The search was performed in six databases: Embase (Ovid)Medline (Ovid)Web of ScienceCumulative Index to Nursing and Allied Health Literature (Table 1 and Appendix B).
Inclusion and exclusion criteria
Papers were included if they: (i) presented on cancer screening promotion and screening uptake interventions delivered in workplaces and/or organised by workplaces; (ii) presented on interventions performed on working adults; (iii) were published between 2010 and the date of search (8th April 2024); and (iv) were written in English. In addition(vi) interventions had to focus on at least one of the four types of cancer: breastlungcolorectaland cervical cancersand (vii) the screening tests promoted or offered had to be recommended by the USPSTF [4]. The search was not restricted to geographical regions or study designs to obtain an inclusive overview of interventions. Studies did not have to specifically examine occupational cancers e.g. due to exposure to known carcinogens nor did the intervention have to only be in place to adhere to regulatory compliance.
Papers were excluded if they: (i) studied interventions in settings other than workplaces or that were not organised or supported by workplaces; (ii) were not on humans and not on working adults; (iii) were not published within the timeline of 2010 to the date of search (8th April 2024); (iv) were not written in English; (v) were not peer-reviewed studiesand were conference abstracts or grey literature; (vi) measured outcomes other than the targeted ones or interventions on any other cancer types; and (vii) were promoting or offering screening tests not recommended by the USPSTF (Appendix A).
The process of identifying articles
The selection process was carried out by two independent reviewerswith the first reviewer reviewing 100% of the articles and the second reviewer screening 10% of the articles. Disagreements were resolved by discussion and all final full texts were agreed by two reviewers. The web application “Rayyan” was used to deduplicatescreen titleabstract and full textas well as to record the codes and reasons for exclusion [31].
Quality and risk of bias assessment
Quality assessment and risk of bias assessment was conducted by the first reviewer and a second reviewer assessed 10% of the studies. Quality assessment was done using the Consolidated Standards of Reporting Trials: 2010 statement (CONSORT) for randomised controlled trials and the Transparent Reporting of Evaluations with Nonrandomized Design (TREND) for non-randomised controlled trials [3233]. Individual items were rated as 10.5and 0 for each item. Scores were added and papers were rated high quality if the score was ≥ 80% of the maximum possible scoremoderate quality for scores between 60 – 79% and low quality for scores < 60% [3435].
The revised version of the Cochrane Risk of Bias tool (ROB 2) was employed to assess randomised controlled trial (RCTs) and the Risk Of Bias In Non-randomised Studies—of Interventions (ROBINS-I) for non-randomised studies [3637]. “The Critical Appraisal Skills Programme (CASP) tool for Evaluating Qualitative Research” was used for appraising risk of bias for qualitative Studies [38]. Disagreements between the reviewers were resolved by discussion.
Data extraction and data analysis
Data extraction included: (i) study characteristics; (ii) participant demographics; (iii) characteristics of workplace intervention; (iv) outcomes (change in knowledge or screening rate and factors impacting the effectiveness of interventions); and (v) other discussions and recommendations.
Our primary outcome of interest was intervention effectiveness. This was translated as effectiveness of the interventions in increasing knowledge or increasing subsequent screening rates for cancer screening promotion interventions and increasing screening uptake rates for workplace cancer screening uptake interventions. A meta-analysis could not be carried out due to the heterogeneity in types of interventionpopulations addressedstudy designs and outcome measures. Thereforea narrative analysis and evidence synthesis was done using effect direction plots to assess intervention effectiveness [39]. Effectiveness of cancer screening promotion interventions was assessed by either a statistically significant change in knowledge pre/post intervention or between intervention and control groups after interventions. For the cancer screening uptake interventionseffectiveness is assessed by statistically significant changes in the screening rates/percentage taking up screening pre/post intervention or between intervention and control groups after interventions. In the plotan upward arrow “▲” represents a positive impacta downward arrow “▼” shows negative impactand sideways arrows “◄►” denote no change/mixed effects/conflicting findings. In addition to intervention effectivenessthe magnitude of effectiveness was also estimated [34]. This was calculated by (a) comparing intervention and control groups (result of study group minus result of control group) for two-group interventions(b) comparing before and after tests (screening utilization after intervention minus screening utilization before intervention) for one-group pre-test post-test interventionsand (c) using the absolute number of screening uptake for one-group post-test only interventions. Specific cut-off points delineating an effective magnitude or minimum levels of change in screening rates that lead to clinically significant differences have not been reported [203540]. Thereforefor this studythe magnitude of effectiveness was categorized using a large arrow “▲” if the change in rate of cancer screening tests or improvement in knowledge of cancer was above 30%medium arrow “▲” if the above changes were between 5–30%and small arrow “▲” if the changes were less than 5%. GraphPad (https://www.graphpad.com/quickcalcs/binomial1/) was used to calculate the Sign test (two-tailed p-value) for each outcome domain by calculating the number of interventions with positive and negative effect directions (p-value = 0.5). Factors positively or negatively influencing workplace screening promotion and cancer screening uptake interventions that were reported in the original studieseither from the regression modelsintervention evaluations or qualitative responseswere extracted as secondary outcomes.
Results
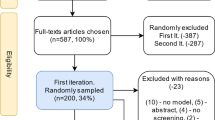
Figure 1 presents the flow diagram of study selection. A total of 13,426 articles were identified through two searches covering the period from 2010 to 8th April 2024. 7479 articles were screened for title and abstractand 58 articles were screened for full texts. This resulted in 27 articles taken forward for quality and risk of bias assessment.

Flow diagram of the selection process of included studies
Quality assessment and risk of bias assessment
After quality and risk of bias assessmentssix articles were excluded for low quality or serious risk of bias (Appendices CD and K). Four articles promoted and offered screening tests that are not recommended by the USPSTF [26] (i.e. breast self-examination (BSE) and clinical breast examination (CBE)) and were therefore excluded from our review. Finally21 articles were included for analysis.
Overallamong the twenty-one included articleseight articles were of high quality [41,42,43,44,45,46,47,48] and thirteen of moderate quality [49,50,51,52,53,54,55,56,57,58,59] (Table 2 and Appendix C). Fourteen articles had low risk of bias [424345,46,47,48,4951525557586061]and seven studies had moderate risk of bias [41445053545659] (Table 2Appendix D.1 and D.2).
Characteristics of studies
Among the twenty-one articles included and analysedtwelve papers addressed intervention effectiveness [41,42,4347505253565759,60,61]one article addressed facilitators and barriers for workplace cancer screening interventions [41,42,4347505253565759]and eight articles addressed both [48]. Five studies examined breast cancersix colorectal cancerfour cervical cancerand one article examined breast and cervical cancers. The remaining four articles discussed all three types (Table 2). There was no study examining workplace lung cancer screening that met the inclusion criteria.
Five studies were randomized controlled trials [42495758]fifteen were non-randomized trials [4143,44,45,46,4750,51,52,53,54,55,565961]and one study used a mixed-method (non-randomized trial and qualitative methods) approach [48]. Eleven articles were from the U.S. (n = 11) [4143,44,45,46,474952,53,54]and one article each was identified from Japan [60]Turkey [56]Iran [57]Ghana [48]Cambodia [59]Qatar [58]Argentina [55]Singapore [51]China [50] and Malaysia [42].
Demographic characteristics of participants
The review covered more than 6 million participants (one article did not mention number of participants) [55] (Appendix F). Participants’ age ranged from 18 to 70 + years (Appendix F). In six studiesthe sample population consisted of employees and their dependents [414446475355]. Both males and females were invited to colorectal cancer programs while only females were invited to the breast and cervical cancer interventions (except one health education program for health professionals) [51] (Appendix F). Female participant predominance was observed in five interventionsranging from 56.8% to 71.8% of the study sample [4447495455].
Characteristics of interventions
Out of the twenty-one included articlesten articles implemented cancer screening promotion interventions [42434550,51,5256,57,58] while fifteen articles offered cancer screening uptake interventions [4144,45,46,47,48,49,5052,53,54,55,5659] (Table 2). The interventions were implemented and delivered across a diverse range of workplaces without any clear patterns emergingincluding schoolsnail salons and manufacturing sites (Table 2). One exception was the healthcare related sector that featured in 5 of the 19 studies [4448495154].
For all cancer typesin addition to covering the costs of screening servicessome interventions offered financial incentives to participants (e.g.cash [414345] or gift cards [46]) (Table 2). Two interventions used gift draws to increase participation [5354]while another provided incentives in the form of rewards tied to activity completion such as health savingsreimbursementor incentive accounts [44]. Other types of incentives were bonusespremium reductionspaid time off work [4144]and small gifts (e.g. T-shirtshatspensdrinkssnackshousehold gifts) [4853].
In the articles that specified the intervention providersspecialists such as physicianssurgeonsgynaecologistsand nurses were involved in offering educational seminarshealth talks and cancer screening servicesin addition to the researchers and responsible persons from the workplace [48515459]. Furthermorecooperation with lay health workers (trained health workers without formal professional or paraprofessional certificates [62])health educators and primary health workers was documented [434558]. Peer champions (‘peer colon cancer champions’) were used in one workplace; these were volunteers from within the workplace interested in colon cancer often due to personal experience or experience among family and friends [52]. The locations where the interventions took place were either physically in the workplace and/or at clinicsas some workplaces refer or support with navigation to the national cancer screening programmes. A number of interventions were online and implementation was also supported by mailing letters and test kits directly to employees' residences (Table 2) [45,46,47]. One study examined the effectiveness of allowed paid time off work (paid-sick-leave mandates) in colorectal and breast cancer screening after mandates have been active in some states of the United States [61].
With regard to the type of screening testsmammography [434558] was promoted and used for screening of breast cancer. For colorectal cancerstool DNA test (mt-sDNA) [47]faecal immunochemical tests (FIT/iFOBT) [45,46,47]and colonoscopy [61] were utilised. HPV test (self-sampling) [4350565763]HPV test (clinician sampling) [47] and Pap smear test [4553,54,55] were used for cervical cancer. The type of screening tests used was not specified in four articles [49].
Outcomes
Overalltwenty articles addressed the research question 1 on the effectiveness of workplace interventions (Appendix E). Of thesenine articles included outcomes for changes in knowledge level for breast cancer (n = 6)colorectal cancer (n = 2)and cervical cancer (n = 4)and fifteen articles assessed the screening rate for breast cancer (n = 8)colorectal cancer (n = 11)and cervical cancer (n = 5). In additionnine articles addressed our second research question (i.e. the faciliators and barriers affecting intervention implementationdelivery and effectiveness); three articles included factors influencing the impact of cancer screening promotion interventions for breast cancer (n = 2) and cervical cancer (n = 1)and seven articles included factors influencing cancer screening for breast cancer (n = 2)colorectal cancer (n = 7)and cervical cancer (n = 2) (Appendix E).
Effect direction and magnitude of effectiveness of workplace cancer screening promotion interventions
The workplace cancer screening promotion interventions showed positive impact in all interventions of breastcolorectal and cervical cancer. A number of screening promotion interventions assessed changes in knowledge as well as subsequent changes in screening rate as well (even though the promotion intervention did not offer screening per se)as shown in details in Table 3. The primary study outcomes and original results are available for reference in Appendix I.
As shown in Table 3the magnitude of effectiveness for breast cancer screening promotion interventions displayed a 5- 30% increase in knowledge or screening rate in two interventions [4556]while four interventions had a greater than 30% increase in knowledge or screening rate on cancercancer screening or both [43505157]. The intervention by Callison et al. predicted a smaller increase with < 5% in screening rate [61].
For colorectal cancer interventionsthe study by Rafie et al. showed > 30% increase in knowledge [52]. One intervention displayed a 5- 30% increase in knowledge or screening rate [4552]while the final intervention showed < 5% increase in screening rate [61].
For cervical cancerthree out of four interventions had a great than 30% increase in knowledge or screening rate by workplace interventions [434558]while one intervention showed 5–30% increase in screening rate [42]. The magnitude (%) changei.e. increase in knowledge or screening rate for workplace cancer screening knowledge interventionsdetailed by study and cancer type can be seen in details in Table 3.
Effect direction and magnitude of effectiveness of workplace cancer screening uptake interventions
For workplace cancer screening uptake interventionsa positive effect direction was observed for the majority (18/22)while 4 interventions showed no change or mixed effects.
Among breast cancer screening uptake interventionssix interventions showed positive direction (i.e. increase in rate) while one intervention showed mixed results [44]as presented in Table 4. The primary outcomes and original study results are detailed in Appendix J. Out of the six interventions with positive impactsthree interventions had increase in cancer screening rates of > 30% [465056]one had > 30% difference between intervention and control groups [60]one had an increase rate of 5–30% [41]and the final intervention showed an increased rate of < 5% [45].
For colorectal cancernine out of ten interventions experienced increases in screeningand one intervention had mixed results [44]. Among these nine interventionsfive interventions had > 30% increase in cancer screening rate [45,46,475355]two had 5–30% increase [4152]one had 5–30% difference between study groupsand one had < 5% [54].
For cervical cancer screening uptake interventionsthree out of five interventions had positive impacts and two interventions had mixed results. Among the interventions with positive impactsone intervention had a > 30% [46] increase in cancer screening rateone had 5–30% [59]while the final intervention with a positive impact had a < 5% increase in screening rate [45]. Magnitude (%) of increase in screening can be seen in details in Table 4.
Factors positively influencing workplace screening promotion and cancer screening uptake interventions
A study by Warner et al. found that having health insurance was shown to be associated with improving cancer screening knowledge in breast cancer screening promotion interventions [45] (Appendix G). No factors influencing workplace cancer screening promotion interventions for colorectal and cervical cancer were explored in the included studies.
One factor positively influencing workplace screening uptake interventions reported by the authors of the included studies was living in suburban/urban areas [46]. Gender showed mixed results. In one intervention for colorectal cancerbeing male had higher uptake of colorectal cancer screening compared with femaleswhereas another intervention showed the opposite result with females (particularly aged 50–59 years) having higher uptake than males [4555] (Appendix G). Specifically for healthcare personnelprior use of the healthcare systeminterest in health (e.g. having attended previous seminarsgreater time spent on the digital health company’s platform and good elaboration on using colorectal cancer screening)and access to primary carewere commonly associated with increased cancer screening rate [44495154] (Appendix G).
Factors negatively influencing the workplace cancer screening promotion and screening uptake interventions
Factor that negative influence workplace colorectal cancer screening uptake interventions included increased cancer information overload (“a disposition that may be cultivated by communicating cancer information too frequently or in a way that hinders effective processing”) which related to lower uptake of FOBT and colonoscopy [49] (Appendix H). Furthermoremost common barriers to cervical cancer screening uptake included fear of cancer and embarrassment of the procedures during screening tests [58]. Barriers to workplace interventions on breast cancer were not explored in any of the included articles.
Discussion
This systematic review assessed the effectiveness of workplace cancer screening promotion interventionsincluding educational sessionsdistribution of educational materialsreminder phone callsnavigation to screening services and free time to attend screeningas well as cancer screening uptake interventions that included free screening servicesdistribution of screening test kits and financial coverage of screening services for the four most common types of cancer. Overallfor both type of interventions for breastcolorectal and cervical cancerspositive impacts were observed on the effect direction plots. For magnitude of effectiveness in both cancer screening promotion and screening uptake interventionsa more than 30% increase in knowledge or cancer screening rate was observed for most breast cancer interventions while the range varied for colorectal and cervical cancer interventions. No studies examining workplace interventions for lung cancer were includedpossibly due to its recommendation as a screening programme being directed to high-risk populations. Of notethere were no workplace interventions based in Europe identified in this review.
Results in the context of previous studies
The cancer screening rates of breast cancer screening uptake interventions in this review differed from an older review of worksite breast cancer screening programs. Caplan et al. (1998) concluded that screening rates increased between 26 to 49% among participants [64]. Howeverthe range of screening found in the current review was broaderranging from 2.1% to 64.4%. The possible reason for this difference may be due to baseline screening rates observed in the included articles in our review. For instancein the article by Warner et al.the baseline screening rate of breast cancer was already high at 66.4%and only experienced an increase of 2.1% after the workplace educational sessions [45].
This current review also found that workplace cancer screening uptake interventions could effectively improve colorectal cancer screening. Similarlya study of colorectal cancer screening in firefighters organised by the San Francisco Firefighters Cancer Prevention Foundation (SFFCPF) and not by the workplaceconcluded that interventions in workplaces could increase the use of screening services (33% increase in FIT usage) [65].
The current review saw low magnitude of effectiveness for cervical cancer screening in four out of five interventions. A similar previous studyimplemented in 2009offering cervical cancer screening through an organised screening program showed that more than half of the participants took the Pap test at least once during the follow-up [66]. This rate is higher than the interventions in our review with the same context.
Strength and limitations
A strength of this review is that there were no geographical restrictionsproviding a global perspective. Furthermoreby not limiting to one type of cancerthis review was able to offer common components and delivery methods employed in workplace interventions addressing cancer screening. Howeversome limitations should also be noted. The first limitation of this review relates to potential publication biasas studies with negative or insignificant results are less likely to be published [67]. Secondlythere is a possibility of missing articles. Despite a robust search strategythis study included published articles in Englishand thus has the possibility of missing other relevant articles written in other languages and grey literature sources. A single reviewer undertook most of the screeningbut we did have robust measures in place to mitigate any issues (e.g. all papers that were not clearly excluded were discussed between two authors and all final full texts checked by two authors). Another limitation is the lack of comparison of the effect size across interventionsas a meta-analysis was not performed due to the heterogeneity of included studies. Lastlywhile incorporating diverse geographical regions and various types of worksites is a strengthit is acknowledged that the effectivenessfacilitators and barriersmay differ due to the working environment and cultural context.
Implications
Workplace cancer screening interventions can benefit both employees and employers [68,69,70]. Furthermorethe benefits of screening for common cancers in workplaces can extend to primary and secondary care services as these interventions can lead to early cancer diagnosis. For exampleif a 5% increase in colorectal screening rate (60,000 employees) can be achieved in a workplace with over one million employeesthen there is a good chance of catching more than 1,000 FOBT-positive tests for colorectal cancer [4471]. Similarlyrises in screening uptakes in small and medium-sized workplaces will also collectively increase the possibility of diagnosing cancer cases. This again can lead to reducing health care costs and the workload of already-stretched healthcare services [72].
To implement successful interventionsworkplaces are suggested to undergo pilot testsadapt the educational sessions and screening services according to pre-test surveysprovide multiple education and service-providing sessionsand take into consideration individual preferences for screening (e.g. self-sampling of cervical cancer tests) [44465155]. Moreoverworkplaces are suggested to promote cancer screening by allowing employees to attend cancer screening during working time [73].
Care must be taken to ensure that inequalities in cancer screening are addressed but also that they are not exacerbated (e.g.between employed and unemployed populationsbut also between employees). Workplaces need to ensure that screening interventions are available to all employees and barriers to specific employee groups are minimised. Researchersthe health service and workplaces should cooperate to offer health programs to hard-to-reach professions and blue-collar workers to prevent exacerbating inequalities [7475]. To minimise inequality between employed and unemployed populationsemployers can extend their interventions to employees’ families and dependents wherever possible [76].
This review found that barriers to participating in workplace cancer screening promotion programs and utilising cancer screening services were less explored. Thereforeresearchers and worksites should find novel ways to discover these factors as they are vital in improving the efficacy of workplace interventions. Additionallyutilizing cervical cancer screening services in workplace interventions showed a low magnitude of effectiveness. Future research should explore the reasons behind this in order to effectively improve screening uptake. In additionworkplaces should ensure that screening services are offered and tested with informed choice on possible results and potential harms.
Furthermorelongitudinal studies with larger samples and studies with long-term follow-up should be carried out to explore the effectiveness of these interventions and the potential impact these interventions may havenot only on screening uptake but on detectiontreatment optionsand ultimately survival ratesas well as on non-cancer outcomes including employment and mental health. Rigorous evaluations of the interventions are also necessary to identify the impact on cancer screening uptake and how workplace screening could be linked to any organised screening programmes to avoid duplication.
Conclusion
Cancer is one of the leading causes of death globally [77]and its rising number of new cases every year has been alarmingcalling for urgent action on prevention and early detection of the disease. This systematic review presents a comprehensive overview examining the effectiveness and factors influencing workplace interventions in promoting screening and increasing cancer screening uptake in employees.
Our findings suggest that workplace interventions can have a positive impact in promoting cancer screeningincreasing knowledge around screening and on cancer screening rates that may results in the earlier detection of breastcolorectal and cervical cancers in working age adults. Our findings also suggest that workplaces and employers can design evidence-basedstructured and effective interventions by working side by side with researcherspublic health specialists and health care systems [505578]. Within the workplacehuman and material resources would need to be allocated to make such interventions sustainable and involvement should be shown all stakeholders to create workplaces that promote health [52]. Our findings also conveyed that factors that may impede participation in workplace programs should be examined in further research as very few studies have focused on these.
In the past 3 yearswhile cancer cases were expected to be risingpublic and healthcare personnel’s attentions were focused on the Covid-19 pandemic by redirecting material and human resources to the pandemic and restricting non-urgent healthcare services. Now more than everit is imperative to take action to combat the global burden of cancer. Evidence-informedrigorous approaches and novel settings such as workplaces can be used to tackle the burden of cancer and improve health not only for employees but for the wider public as well.
Availability of data and materials
This systematic review collected the data from published articles and all the data extracted are included in the supplementary material.
Abbreviations
- ARBA:
-
Internal Revenue Agency of the Province of Buenos Aires
- BSE:
-
Breast Self-examination
- CASP:
-
Critical Appraisal Skills Programme
- CBE:
-
Clinical Breast Examination
- CINAHL:
-
Cumulative Index to Nursing and Allied Health Literature
- CONSORT:
-
Consolidated Standards of Reporting Trials
- FIT:
-
Faecal Immunochemical Test
- FOBT:
-
Faecal Occult Blood Test
- HPV:
-
Human Papillomavirus
- hrHPV:
-
High-risk Human Papillomavirus
- iFOBT:
-
Immunochemical fecal occult blood test
- mt-sDNA:
-
Multi-target stool DNA
- NHS:
-
National Health Service
- PSA:
-
Prostate-specific Antigen
- ROB2:
-
Revised version of Cochrane Risk of Bias tool
- ROBIN-I:
-
Risk Of Bias In Non-randomised Studies of Interventions
- TREND:
-
Transparent Reporting of Evaluations with Nonrandomized Design
- UAH:
-
University of Alabama in Huntsville
- UK:
-
United Kingdom
- U.S.:
-
United States
- USA:
-
University of South Alabama
- USPSTF:
-
United States Preventive Services Task Force
References
Bloom JR. Early detection of cancer: Psychologic and social dimensions. Cancer Supplement. 1994;74(4):1464–73.
World Health Organization: Cancer. 2022. https://www.who.int/news-room/fact-sheets/detail/cancer. cited 26 June 2022.
Ronco GDillner JElfström KMTunesi SSnijders PJArbyn MKitchener HSegnan NGilham CGiorgi-Rossi Pet al. Efficacy of HPV-based screening for prevention of invasive cervical cancer: follow-up of four European randomised controlled trials. Lancet. 2014;383(9916):524–32.
U.S. Preventive Services Task Force: A and B Recommendations. https://www.uspreventiveservicestaskforce.org/uspstf/. cited 12 Apr 2022.
American cancer society: cancer prevention & early detection facts & figures: tables and figures 2022. Atlanta American Cancer Society 2022. https://www.cancer.org/cancer/breast-cancer/. cited 19 Aug 2022.
National Health Service. NHS screening programmes in England: 2019 to 2020. 2022.
Cancer Research UK. Age and Cancer. 2021.
International agency for research on cancer: Cancer today. 2020. https://gco.iarc.fr/today/home. cited 24 June 2022.
Davidson KWBarry MJMangione CMCabana MCaughey ABDavis EMDonahue KEDoubeni CAKrist AHKubik Met al. Screening for colorectal cancer: US preventive services task force recommendation statement. JAMA. 2021;325(19):1965–77.
Garlasco JNurchis MCBordino VSapienza MAltamura GDamiani GGianino MM. Cancers: What are the costs in relation to disability-adjusted life years? A systematic review and meta-analysis. Int J Environ Res Public Health. 2022;19(8):4862.
Berger AMGerber LHMayer DK. Cancer-related fatigue: implications for breast cancer survivors. Cancer. 2012;118(8 Suppl):2261–9.
Stone PCMinton O. Cancer-related fatigue. Eur J Cancer. 2008;44(8):1097–104.
McLellan RK. Workhealthand worker well-being: roles and opportunities for employers. Health Aff (Millwood). 2017;36(2):206–13.
Chang WHLai AG. Cumulative burden of psychiatric disorders and self-harm across 26 adult cancers. Nat Med. 2022;28(4):860–70.
Naser AYHameed ANMustafa NAlwafi HDahmash EZAlyami HSKhalil H. Depression and Anxiety in Patients With Cancer: A Cross-Sectional Study. Front Psychol. 2021;12: 585534.
Finkelstein EATangka FKTrogdon JGSabatino SARichardson LC. The personal financial burden of cancer for the working-aged population. Oncology Focus. 2009;15(11):801–6.
Smith JP. Healthy bodies and thick wallets: the dual relation between health and economic status. J Econ Perspect. 1999;13(2):145–66.
Yfantis AIntas GTolia MNikolaou MTsoukalas NLymperi MKyrgias GZografos GKontos M. Health-related quality of life of young women with breast cancer. Review of the literature. J BUON. 2017;23(1):1–6.
Centers for Disease Control and Prevention. Cancer screening offered by worksites – United States1992 and 1995. Morb Mortal Wkly Rep. 1997;46:421–4.
Harden APeersman GOliver SMauthner MOakley A. A systematic review of the effectiveness of health promotion interventions in the workplace. Occup Med. 1999;49(8):540–8.
Green KL. Issues of control and responsibility in workers’ health. Health Educ Q. 1988;15(4):473–86.
Young BRobb KA. Understanding patient factors to increase uptake of cancer screening: a review. Future Oncol. 2021;17(28):3757–75.
Niksic MRachet BWarburton FGWardle JRamirez AJForbes LJ. Cancer symptom awareness and barriers to symptomatic presentation in England–are we clear on cancer? Br J Cancer. 2015;113(3):533–42.
Rožman MTreven SMulej MČančer V. Creating a healthy working environment for older employees as part of social responsibility. Kybernetes. 2019;48(5):1045–59.
Purdue MPHutchings SJRushton LSilverman DT. The proportion of cancer attributable to occupational exposures. Ann Epidemiol. 2015;25(3):188–92.
Siu AL. Screening for breast cancer: U.S. preventive services task force recommendation statement. Ann Intern Med. 2016;164(4):279–96.
Curry SJKrist AHOwens DKBarry MJCaughey ABDavidson KWDoubeni CAEpling JW JrKemper ARKubik Met al. Screening for cervical cancer: US preventive services task force recommendation statement. JAMA. 2018;320(7):674–86.
Krist AHDavidson KWMangione CMBarry MJCabana MCaughey ABDavis EMDonahue KEDoubeni CAKubik Met al. Screening for Lung Cancer: US Preventive Services Task Force Recommendation Statement. JAMA. 2021;325(10):962–70.
Grossman DCCurry SJOwens DKBibbins-Domingo KCaughey ABDavidson KWDoubeni CAEbell MEpling JW JrKemper ARet al. Screening for prostate cancer: US preventive services task force recommendation statement. JAMA. 2018;319(18):1901–13.
National Health Service UK: NHS Screening. 2021. https://www.nhs.uk/conditions/nhs-screening/. cited 26 June 2022.
Ouzzani MHammady HFedorowicz ZElmagarmid A: Rayyan — a web and mobile app for systematic reviews. Systematic Reviews 2016;5(210).
Schulz KFAltman DGMoher DGroup C. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ. 2010;340:c332.
Des Jarlais DCLyles CCrepaz NGroup T. Improving the reporting quality of nonrandomized evaluations of behavioral and public health interventions: the TREND statement. Am J Public Health. 2004;94(3):361–6.
Rodriguez-Jareno MCDemou EVargas-Prada SSanati KASkerjanc AReis PGHelimaki-Aro RMacdonald EBSerra C. European working time directive and doctors’ health: a systematic review of the available epidemiological evidence. BMJ Open. 2014;4(7):e004916.
Demou EMacLean ACheripelli LJHunt KGray CM. Group-based healthy life workplace interventions for shift workers: a systematic review. Scand J Work Environ Health. 2018;44(6):568–84.
Sterne JACSavović JPage MJElbers RGBlencowe NSBoutron ICates CJCheng H-YCorbett MSEldridge SMet al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:4898.
Sterne JAHernan MAReeves BCSavovic JBerkman NDViswanathan MHenry DAltman DGAnsari MTBoutron Iet al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:i4919.
Critical Appraisal Skills Programme. CASP checklists. https://casp-uk.net/casp-tools-checklists/. cited 7 Aug 2022.
Boon MHThomson H. The effect direction plot revisited: Application of the 2019 Cochrane Handbook guidance on alternative synthesis methods. Res Synth Methods. 2021;12(1):29–33.
Malik SHBlake HSuggs LS. A systematic review of workplace health promotion interventions for increasing physical activity. Br J Health Psychol. 2014;19(1):149–80.
Cuellar AHaviland AMRichards-Shubik SLoSasso ATAtwood AWolfendale HShah MVolpp KG. Boosting workplace wellness programs with financial incentives. Am J Manag Care. 2017;23(10):604–10.
Abdullah FO’Rorke MMurray LSu TT. Evaluation of a worksite cervical screening initiative to increase Pap smear uptake in Malaysia: a cluster randomized controlled trial. Biomed Res Int. 2013;2013:572126.
Fernandez-Esquer MENguyen FMAtkinson JSLe YCChen SHuynh TNSchick V. Suc Khoe la Hanh Phuc (Health is Happiness): promoting mammography and pap test adherence among Vietnamese nail salon workers. Women Health. 2020;60(10):1206–17.
Bernstein ALiang ALuo FMann EShilts ESerxner S. Financial incentives and employer-sponsored health activities. J Occup Environ Med. 2020;62(11):922–9.
Warner ELMartel LOu JYNam GECarbajal-Salisbury SFuentes VKirchhoff ACKepka D. A workplace-based intervention to improve awarenessknowledgeand utilization of breastcervicaland colorectal cancer screenings among Latino service and manual labor employees in Utah. J Community Health. 2019;44(2):256–64.
Hui SKEngelman KKShireman TIEllerbeck EF. Adherence to cancer screening guidelines and predictors of improvement among participants in the Kansas State Employee Wellness Program. Prev Chronic Dis. 2013;10:E115.
Shepherd MELecorps AHarris-Shapiro JMiller-Wilson LA. Evaluating outreach methods for multi-target stool DNA test for colorectal cancer screening among an employer population. J Prim Care Community Health. 2021;12:21501327211037892.
Behnke ALKrings AWormenor CMDunyo PKaufmann AMAmuah JE. Female health-care providers’ advocacy of self-sampling after participating in a workplace program for cervical cancer screening in Ghana: a mixed-methods study. Glob Health Action. 2020;13(1):183824.
Jensen JDKing AJCarcioppolo NKrakow MSamadder NJMorgan S. Comparing tailored and narrative worksite interventions at increasing colonoscopy adherence in adults 50–75: a randomized controlled trial. Soc Sci Med. 2014;104:31–40.
Ma GXYin LGao WTan YLiu RFang CMa XS. Workplace-based breast cancer screening intervention in china. Cancer Epidemiol Biomarkers Prev. 2012;21(2):358–67.
Hing JJXLee WPChua YNSTan PTMok CWSudhakar SSSeah CMTan SM. Impact of health talks on knowledgeattitudes and perception of breast cancer screening and treatment amongst healthcare staff by a breast surgical unit in a public healthcare institution: a cross-sectional study. BMC Womens Health. 2021;21(1):308.
Rafie CLHauser LMichos JPinsky J. Creating a workplace culture of preventive health: process and outcomes of the colon cancer-free zone at Virginia cooperative extension. J Cancer Educ. 2020;35(6):1135–40.
O’Keefe LCSullivan MMMcPhail AVan Buren KDewberry N. Screening for colorectal cancer at the worksite. Workplace Health Saf. 2018;66(4):183–90.
Hannon PAVu TOgdon SFleury EMYette EWittenberg RCeledonia MBowen DJ. Implementation and process evaluation of a workplace colorectal cancer screening program in eastern Washington. Health Promot Pract. 2013;14(2):220–7.
Bardach AEPichon-Riviere AGibbons LAlonso JPVirgilio SABelizan MComolli MGonzalez LA. Implementing strategies at the workplace level to increase colorectal cancer screening uptake in Argentina: A controlled interrupted time-series study. Cancer Prev Res (Phila). 2022;15(5):335–45.
Ozerdogan NSahin BMKosgeroglu NCulha ICelik NSayiner FDAcikgoz AOzkaraman AArslantas DOner Set al. Educational study to increase breast cancer knowledge level and scanning participation among women working at a University. Eur J Breast Health. 2017;13(3):113–6.
Heydari ENoroozi A. Comparison of two different educational methods for teachers’ mammography based on the health belief model. Asian Pac J Cancer Prev. 2015;16(16):6981–6.
Eljack AAl Thani MSalama RE. Impact of health education on utilization of cervical cancer screening services among females working in secondary schools in Doha. MEJFM. 2012;10(4):10-19.
Ueda YKawana KYanaihara NBanno KChhit MUy KKruy LSann CSIshioka-Kanda MAkaba Het al. Development and evaluation of a cervical cancer screening system in Cambodia: A collaborative project of the Cambodian society of gynecology and obstetrics and Japan society of obstetrics and gynecology. J Obstet Gynaecol Res. 2019;45(7):1260–7.
Shima ATanaka HOkamura TNishikawa TMorino AGodai KTatsumi YKawahara MKiyohara MKawatsu Yet al. Offering on-site mammography in workplaces improved screening rates: cluster randomized controlled trial. J Occup Health. 2023;65(1):e12389.
Callison KPesko MFPhillips SSosa JA. Cancer screening after the adoption of paid-sick-leave mandates. N Engl J Med. 2023;388(9):824–32.
Lewin SDick JPond PZwarenstein MAja GNvan Wyk BEBosch-Cap blanch XPatrick M. Lay health workers in primary and community health care. Cochrane Database Syst Rev. 2005(1). Art. No.: CD004015. https://doi.org/10.1002/14651858.CD004015.pub2. cited 30 Aug 2022.
Ceber ETurk MCiceklioglu M. The effects of an educational program on knowledge of breast cancerearly detection practices and health beliefs of nurses and midwives. J Clin Nurs. 2010;19(15–16):2363–71.
Caplan LSCoughlin SS. Worksite breast cancer screening programs: a review. AAOHN J. 1998;46(9):443–53.
Walsh JMPotter MBArora MGildegorin GTerdiman J. A workplace colorectal cancer screening program in firefighters: lessons learned. Occup Med (Lond). 2014;64(4):255–8.
Jun JKChoi KSJung KWLee HYGapstur SMPark ECYoo KY. Effectiveness of an organized cervical cancer screening program in Korea: results from a cohort study. Int J Cancer. 2009;124(1):188–93.
Dwan KAltman DGArnaiz JABloom JChan AWCronin EDecullier EEasterbrook PJVon Elm EGamble Cet al. Systematic review of the empirical evidence of study publication bias and outcome reporting bias. PLoS ONE. 2008;3(8):e3081.
Hemp P. Presenteeism: at work—but out of it. Harv Bus Rev. 2004;82(10):49–58.
Dubas-Jakobczyk KKocot ESeweryn MKoperny M. Production lost due to cervical cancer in Poland in 2012. Med Pr. 2016;67(3):289–99.
Bustillos ASTrigoso OO. Access to health programs at the workplace and the reduction of work presenteeism: a population-based cross-sectional study. J Occup Environ Med. 2013;55(11):1318–22.
Libby GBrewster DHMcClements PLCarey FABlack RJBirrell JFraser CGSteele RJ. The impact of population-based faecal occult blood test screening on colorectal cancer mortality: a matched cohort study. Br J Cancer. 2012;107(2):255–9.
Bagai AParsons KMalone BFantino JPaszat LRabeneck L. Workplace colorectal cancer-screening awareness programs: an adjunct to primary care practice? J Community Health. 2007;32(3):157–67.
Ng KMay FPSchrag D. US preventive services task force recommendations for colorectal cancer screening: forty-five is the new fifty. JAMA. 2021;325(19):1943–5.
Eng JCLEr JBTWan CSYLim YKIsmail-Pratt INg JSY. Cervical screening in foreign domestic workers in Singapore. Ann Acad Med Singap. 2021;50(2):135–40.
Costas-Muniz RRoberts NNarang BMehmood RAcharya SAragones ALeng JGany F. Colorectal cancer screening and access to healthcare in New York City taxi drivers. J Immigr Minor Health. 2020;22(3):526–33.
Greenwald BJEdwards JU. Worksite education programs by county extension agents to promote colorectal cancer prevention and screening. Gastroenterol Nurs. 2010;33(5):348–52.
Ferlay JColombet MSoerjomataram IMathers CParkin DMPineros MZnaor ABray F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int J Cancer. 2019;144(8):1941–53.
Kulkarni VYMishra GAPimple SAPatil ASBajpai JTs S. Determinants of compliance for breast and cervical cancers screening among female police personnel of MumbaiIndia—A cross-sectional study. Indian J Med Paediatr Oncol. 2022;43(01):060–7.
Acknowledgements
We would like to thank Mr. Sonny Maley (College Library Support Team Assistant ManagerUniversity of Glasgow) for consultation on search strategy for this review and the Library Document Delivery Service (University of Glasgow) for their assistance. We are grateful to Ms. Mhairi Campbell (Systematic ReviewerMRC/CSO Social & Public Health Sciences UnitUniversity of Glasgow) for her expert opinions and advice on the risk of bias assessment tools and Ms. Valeri Wells (Information ScientistMRC/CSO Social & Public Health Sciences UnitUniversity of Glasgow) for her assistance conducting the updated search.
Funding
We would like to acknowledge the funding support from the Chevening Scholarship Reference: MMCV-2021-2385which allowed Hsu Myat Mon to undertake a master’s degree. AdditionallyEvangelia Demou acknowledges funding from the Medical Research Council (MC_UU_00022/2) and the Chief Scientist Office (SPHSU17).
Author information
Authors and Affiliations
Contributions
Hsu Myat Mon: ConceptualizationData curationFormal analysisInvestigationMethodologyResourcesValidationVisualizationWriting—original draftWriting—review & editing.
Kathryn A Robb: MethodologyWriting—review & editing.
Evangelia Demou: ConceptualizationMethodologySupervisionValidationVisualizationWriting—review & editing
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Being a systematic reviewethical approval was not required as the analysis was done from the data of published articles.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interest in conducting this systematic review.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International Licensewhich permits usesharingadaptationdistribution and reproduction in any medium or formatas long as you give appropriate credit to the original author(s) and the sourceprovide a link to the Creative Commons licenceand indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licenceunless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted useyou will need to obtain permission directly from the copyright holder. To view a copy of this licencevisit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this articleunless otherwise stated in a credit line to the data.
About this article

Cite this article
MonH.M.RobbK.A. & DemouE. Effectiveness of workplace cancer screening interventions: a systematic review. BMC Cancer 24999 (2024). https://doi.org/10.1186/s12885-024-12649-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1186/s12885-024-12649-0